Five main types of Thyroid Cancer
- Papillary Carcinoma (80%)
- Follicular Carcinoma (10%)
- Medullary Carcinoma (5%)
- Hurthle Cell Carcinoma (4%)
- Anaplastic/Undifferentiated Carcinoma (1-2%)
P’s of Papillary Thyroid Cancer:
- Popular (most common type – 80%)
- Psammoma bodies
- Palpable Lymph Nodes – common
- Positive Iodine 131 uptake
- Positive Prognosis
- Postoperative Iodine 131 to diagnose / treat metastasis if a total thyroidectomy was done.
F’s of Follicular Cancer of the Thyroid
- Far away metastasis (spreads hematogenously)
- FNA NOT (FNA cannot be done to diagnosis Follicular Cancer of the thyroid
- Female predominance (3:1)
M’s of Medullary Cancer of the Thyroid
- MEN II (Multiple Endocrine Neoplasia type II)
- aMyloid
- Median Lymph Node dissection
- Modified neck dissection if lateral nodes are positive
- Secretes Calcitonin
- Stimulated by Pentagastrin
- Cancer of the Thyroid C cells = parafollicular cells
Calcitonin (tumor marker for MTC)
- Reduces blood levels of Calcium
- Opposed the effects of PTH (parathyroid hormone)
- Calcitonin is used as a tumor marker for medullary thyroid cancer (MTC)
Pentagastrin
- Pentagastrin has effects like gastrin
- Pentagastrin is used as a stimulation test to elevate serotonin levels and cause symptoms of carcinoid syndrome, provoking flushing.
- Pentagastrin has been used to stimulate ectopic gastric mucosa for the detection of Meckels diverticulum by nuclear medicine.
- Pentagastrin-stimulated calcitonin test is a diagnostic test for MTC (Medullary carcinoma of the thyroid). In patients with suspected MTC but borderline levels of calcitonin, injecting pentagastrin will cause calcitonin levels to rise tremendously.
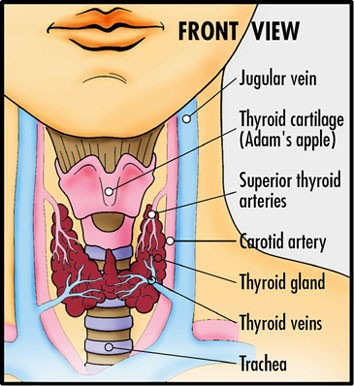
Picture from: http://www.washingtonendocrineclinic.com/Thyroid-Care.html